
Advises Ms. Dimitra Moschou, Special. Rheumatology
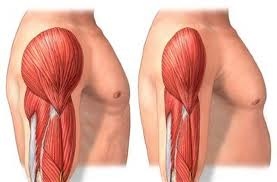
What is sarcopenia?
We should first mention that muscle mass and strength vary throughout life. In general, muscle mass and strength increase with adulthood, are maintained in middle life and then decrease with age. In adulthood up to 40 years are reached the maximum levels, which are higher in men than in women. After the age of 50, a loss of muscle mass of 1-2% per year and a loss of strength of 1.5-5% per year have been reported. In 2010 a new group of representatives (European Group on Sarcopenia in Older People – EWGSOP) set the definition of sarcopenia. According to him, sarcopenia is characterized by progressive and generalized loss of skeletal muscle mass and strength with the risk of serious side effects, such as physical disability, poor quality of life and death. The EWGSOP recommends the simultaneous presence of low muscle mass, low muscle strength and performance for the diagnosis of sarcopenia.
What is the stage of sarcopenia?
The staging of sarcopenia reflects the severity of the condition. The EWGSOP proposes the recognition in:
“Pre-sarcopenia” characterized by low muscle mass without affecting muscle strength or physical performance
“Sarcopenia” characterized by low muscle mass in combination with low muscle strength or low physical performance and
“Severe sarcopenia” where it is characterized by low muscle mass, low muscle strength and low physical performance.
What are the causes of sarcopenia?
In some people, sarcopenia is largely due to aging. In many cases, however, other causes can be identified. Sarcopenia is considered primary when it is related to age or when no other specific cause is obvious, while it is considered secondary when causes other than aging are evident such as a systemic disease.
Physical inactivity also contributes to the development of sarcopenia, either due to a sedentary lifestyle or due to immobility or disability associated with conditions such as dementia and stroke. Further sarcopenia can be developped as a result of insufficient protein intake, which can be due to either anorexia or malabsorption syndrome. The causes of sarcopenia are generally considered to be multifactorial such as: environmental reasons, chronic diseases, chronic inflammation, mitochondrial dysfunction, apoptosis, oxidative stress and hormonal changes.
When do we investigate sarcopenia?
In clinical practice, the investigation of cases can begin when a patient reports symptoms or signs of sarcopenia e.g. fall, feeling of weakness, slow walking speed, difficulty getting up from a chair, weight loss, and muscle loss. In such cases further screening for sarcopenia is recommended.
How is sarcopenia diagnosed?
The parameters of sarcopenia are considered to be muscle mass, muscle strength and physical performance.
Methods for determining muscle strength
Muscle strength can be measured by fist tightening force, using a hand-held dynamometer, usually a jamar type. This method is simple and low cost. Low measurement is a strong predictor of poor mobility and low muscle mass. Due to its ease of use, it consists of hospital practice and community health care. The chair test can be used to assess the muscular strength of the lower limb muscles. The chair test measures the time it takes for a patient to sit 5 times from a sitting position to an upright position without using his or her hands. The chair seat time test is a variation that measures how many times a patient can get up and sit in a chair in 30 seconds.
Methods for determining muscle mass
The X-ray dual energy beam absorption method known as DEXA. It is a widely available tool for determining muscle mass. The advantage of DEXA is that it can provide an estimate of muscle mass in a few minutes with very small doses of radiation. One disadvantage is that it does not have portable equipment for use in the community and its measurements can be affected by the patient’s dehydration status.
Magnetic resonance imaging (MRI) and computed tomography (CT) scans are considered useful methods for non-invasive estimation of muscle mass. However, these tools are not commonly used in primary care due to their high cost, lack of portability and complexity in handling them.
Bioelectric impedance analysis (BIA) has been investigated to estimate muscle mass. Its equipment calculates the volume of lean muscle and fat mass. The BIA has a relatively low cost, is simple to use with readily available results and is suitable for both ambulatory and bedridden patients.
Anthropometric measurements are based on calculating the waist circumference of the upper limb and the thickness of the skin fold and have been used to calculate muscle mass in walking individuals.
Ultrasound is a widely used research technique for estimating muscle mass, locating muscle loss, and evaluating muscle quality. It is a reliable and valid measure and is starting to be used by trained clinicians.
Methods for determining physical performance
This is the Short Physical Performance Battery (SPPB) method, which evaluates a person’s gait speed, balance, strength and endurance. It examines his ability to stand with his feet together, with one foot next to the other, with one foot in front of the other, the time it takes to walk 4 meters, and the time it takes to get up from a chair and the time required to get up from a chair and return to a sitting position 5 times. The maximum score is 12 points and a score below and equal to 8 points indicates poor physical performance.
Walking speed is considered a fast, safe and extremely reliable test for sarcopenia and is widely used in clinical practice. Walking speed has been shown to predict the adverse effects associated with sarcopenia such as falls, disabilities and mortality. A commonly used gait speed test is called a “Standard 4-Meter Walking Speed Test” with a speed measured either manually, with a timer, or with an electronic gauge timer.
Is there a cure for sarcopenia?
Many therapeutic interventions have been tried in an effort to improve the quality or quantity of skeletal mass. These can be divided into 3 major categories that include exercise, diet, and drug substitution. Both aerobic and resistance exercise can improve the rate of decline in muscle mass and strength with age.
Is there prevention?
While genetic and lifestyle factors can accelerate muscle weakness to disability, interventions including diet and exercise seem to slow down these processes. Therefore, to prevent or delay sarcopenia, the goal is to maximize muscle in young adulthood, maintain muscle in middle age, and minimize loss in old age.